Health Care Access and Insurance Availability in Nevada*
Introduction
According to the Institute of Medicine (IOM),
- Approximately 18,000 Americans die prematurely every year, solely because they lack health insurance coverage (Institute of Medicine, 2004).
- The IOM estimates that the aggregate cost of increased morbidity and mortality due to un-insurance in the U.S. is between $65 billion and $130 billion per year.
- Costs to the health care system can be measured conservatively in terms of the value of uncompensated care provided to the uninsured, estimated at almost $35 billion in 2001, of which $24 billion was provided by hospitals.
Access to medical care is not a constitutional right in the U.S., except for prison inmates. Due to the prohibitive costs of medical care and prescription drugs, the majority of Americans cannot afford to pay for health care out-of-pocket. Access to health care requires health insurance coverage. The U.S. health insurance system can be divided into two categories, (1) private insurance programs and (2) government insurance programs (U.S. Census Bureau, 2005):
Individual coverage can be directly purchased from private health insurance companies. Group coverage is provided by health plans offered by an employer or union. Group coverage is generally less expensive than individual coverage. Often, the employer will subsidize a portion of the health insurance premium and the employee pays the remainder. Private health insurance plans are regulated by state health insurance agencies. Over half of larger businesses in this country have self funded employee health insurance plans that are exempt from state insurance regulation.
Coverage is also provided by health plans funded by the federal, state, or local government for certain populations. The major categories of government-funded health insurance are:
- Medicare, http://www.medicare.gov/, is a federal program enacted in 1965 by the Social Security Act. Medicare is the national health insurance program for people age 65 and older. Some people under age 65 with disabilities and people with end-stage renal disease are also covered.
- Medicaid, http://www.cms.hhs.gov/medicaid/default.asp, is a federal program enacted in 1965 that is administered at the state level. It provides medical assistance for the needy, including low-income individuals and families. Coverage is also extended to the aged, blind or disabled. Individual state programs establish income and other eligibility criteria.
- State Children’s Health Insurance Program (SCHIP), http://www.cms.hhs.gov/schip/, is a new children’s health insurance program created under Title XXI of the Social Security Act by The Balanced Budget Act of 1997, http://www.cms.hhs.gov/healthplans/bba/. This program enables states to initiate and expand health insurance coverage for uninsured children.
Most Americans are covered by private insurance obtained through their employers or directly purchased from a private insurance company.
- Government funded insurance programs cover 27% of Americans. Over 15% of all Americans lack any kind of health insurance coverage (DeNavas and Proctor, 2005) (see Figure 1).
The following Federal laws and regulations pertain to the uninsured:
Disproportionate Share Hospital (DSH) Payments, http://www.cms.hhs.gov/dsh/default.asp. Additional payments through the Medicare and Medicaid programs that help hospitals (primarily public and non-profit) finance care to low-income and uninsured patients.
Health Insurance Flexibility and Accountability Initiative (HIFA), http://www.cms.hhs.gov/hifa/default.asp. This is an initiative by a Center for Medicaid and Medicare Services (CMS) that allows states to experiment with different approaches to covering their uninsured population with Section 1115 Medicaid and HIFA waivers.
Health Insurance Portability and Accountability Act of1996 (HIPAA), http://www.cms.hhs.gov/hipaa/. Title I of HIPAA protects health insurance coverage for workers and their families when they change or lose their jobs.
Health Services Resources Agency (HRSA) State Planning Grants, http://www.hhs.gov/grants/index.shtml. HRSA Planning Grants allow states to study their demographic and state insurance trends in order to develop coverage options.
The Consolidated Omnibus Budget Reconciliation Act of 1986 (COBRA) – The law amends the Employee Retirement Income Security Act (ERISA), the Internal Revenue Code and the Public Health Service Act to provide continuation of group health insurance coverage that otherwise may be terminated.
The Personal Responsibility and Work Opportunity Reconciliation Act of 1996, http://www.acf.dhhs.gov/programs/ofa/prwora96.htm. The Act made significant changes to the eligibility of immigrants for Medicaid and SCHIP. Only citizens and “qualified aliens” are eligible for Medicaid or SCHIP benefits. Certain immigrants who entered the United States on or after August 22, 1996 are barred from Medicaid and SCHIP benefits for five years.
Trade Act of 2002, http://www.doleta.gov/tradeact/2002act_index.cfm. The Act provides $12 billion over 10 years in Trade Adjustment Assistance (TAA) to workers who lose their jobs due to trade. The law created the Health Coverage Tax Credit, http://www.irs.gov/individuals/article/0,,id=109960,00.html, a refundable and advanceable tax credit to cover 65% of health insurance premiums of workers covered by the Act. The law also established a tax credit for retirees age 55 or older who receive pensions from the Pension Benefit Guarantee Corporation, http://www.pbgc.gov/.
Uninsured in the U.S.
According to the U.S. Census Bureau definition, a person is considered uninsured if he or she had no health care coverage for the entire year. The following is an overview of the uninsured population in the U.S. (DeNavas and Proctor, 2005; Institute of Medicine, 2004; The Kaiser Commission on Medicaid and the Uninsured, 2005; National Coalition of Health Care, 2004):
- In 2003-2004, the U.S. Census Bureau estimated that, almost 46 million people were uninsured.
- The Congressional Budget Office (CBO) estimated that 60 million people were without insurance at some time during 2003.
- The number of uninsured under age 65 increased by nearly six million between 2000 and 2004, primarily due to a decline in employer-sponsored insurance.
- The number of non-elderly, adult uninsured in America has continued to increase.
- The number of uninsured children has not grown due to expanded coverage under Medicaid and SCHIP.
- The U.S. is the only wealthy, industrialized nation that does not provide publicly funded, universal health insurance coverage.
Five key, overlapping demographic and socioeconomic groups are more likely to be uninsured: (DeNavas and Proctor, 2005; The Kaiser Commission on Medicaid and the Uninsured, 2005; National Coalition of Health Care, 2004):
The Working Uninsured
- In 2003-2004, over 80% of the uninsured come from working families.
- In 2003-2004, 27 million workers were uninsured – 77% held full-time jobs, 56% earned less than $20,000 per year, and 49% were self-employed or worked for small businesses.
- Workers at greater risk of being uninsured are those employed in small businesses, service industries, and blue-collar jobs.
The poor
- In 2003-2004, two-thirds of all uninsured persons were low income Americans (incomes less than 200% of the federal poverty level or about $39,000 a year for a family of four).
- In 2003-2004, 40% of the uninsured had incomes that exceeded eligibility limits of public health insurance programs, such as Medicaid and SCHIP.
Children and Young Adults
- In 2003-2004, 8.3 million children under 18 years old did not have health insurance.
- In 2003-2004, children in poverty (<100% FPL) were more likely to be uninsured than all children.
- In 2003-2004, young adults (18-24 years old) were the most likely of any age group to be uninsured – 30.2%. Young adults are uninsured, because they have low paying jobs without insurance benefits; they are in school and no longer covered by their parent’s insurance; and/or they lose their public coverage when they reach 19 years.
Ethnic and Racial Minorities
Minorities are more likely to be uninsured than whites. The 3 year average (2002-2004) for people without health insurance coverage by race and Hispanic origin were:
- Whites – 11%, Asians - 18%, African Americans – 19.8%, Native Hawaiian and other Pacific Islander – 21.8%, American Indian and Alaska Natives – 29%, and Hispanics – 32.7%.
Higher rates of uninsured among racial and ethnic minorities reflect fewer jobs with insurance coverage, lower family incomes, and a lower number of persons born in the U.S.
Immigrants and Foreign Born Citizens
- Immigrants are much more likely to be uninsured than native-born residents. However, insurance coverage for immigrants increases with length of residency.
- In 2002-2004, 33.7% of residents born outside the U.S. were uninsured. Non-citizens were more likely than naturalized citizens to lack coverage – 44.1 % compared with 17.2%.
Health Care Access and Health Status
The uninsured have less access to needed care, and they experience poorer health (Institute of Medicine, 2004; National Coalition on Health Care, 2004).
- Uninsured adults have a higher risk of dying before age 65 than insured adults.
- Uninsured adults are less likely to receive needed care for serious medical conditions.
- The uninsured are less likely to receive preventive care
- The uninsured are diagnosed at more advanced disease stages.
- Uninsured children are less likely to access routine well-child care, immunizations and dental care.
- Uninsured women are less likely to access prenatal care and newborn care.
- The uninsured are less likely to fill drug prescriptions and are more likely to forego recommended medical tests and treatments due to cost.
- Almost 20% of the uninsured say their usual source of care is the emergency room.
- The uninsured are more likely to be hospitalized for avoidable health conditions, if preventive care had been received.
Uninsured in Nevada
Nevada has one of the higher rates of non-elderly uninsured in the country.
- In 2003-2004, 19% of Nevada non elderly residents were uninsured compared to the national average of 16% (Kaiser Commission on Medicaid and the Uninsured, 2005).
- In 2003-2004, Nevada ranked 6th highest in the nation for the percentage on non insured persons under age 65 (Benedict, 2006).
- In 2001, Nevada ranked 12th highest in the nation for the percentage of non elderly uninsured persons (Association of Retired Persons, 2003).
- In 2001, Texas, New Mexico and Louisiana were the three states with the highest percentage of uninsured persons in the U.S., and Iowa, Wisconsin, and Minnesota, were the 3 states with the lowest percentage of uninsured persons in the U.S. (Association of Retired Persons, 2003).
- The percentage of uninsured non elderly Nevadans has been higher than the national average every year since 1990, except for 1996, when it was equal to the national average (Great Basin Primary Care Association, 2005).
Nevada also has relatively high rates of uninsured low income persons, children, and minority/ethnic residents.
- In 2003-2004, 39% of the low-income (less than 200% of poverty) non-elderly in Nevada were uninsured. The national average was 33%. In 2001, Nevada ranked 16th highest in the nation for the percentage of uninsured adults with family income below the national median income.
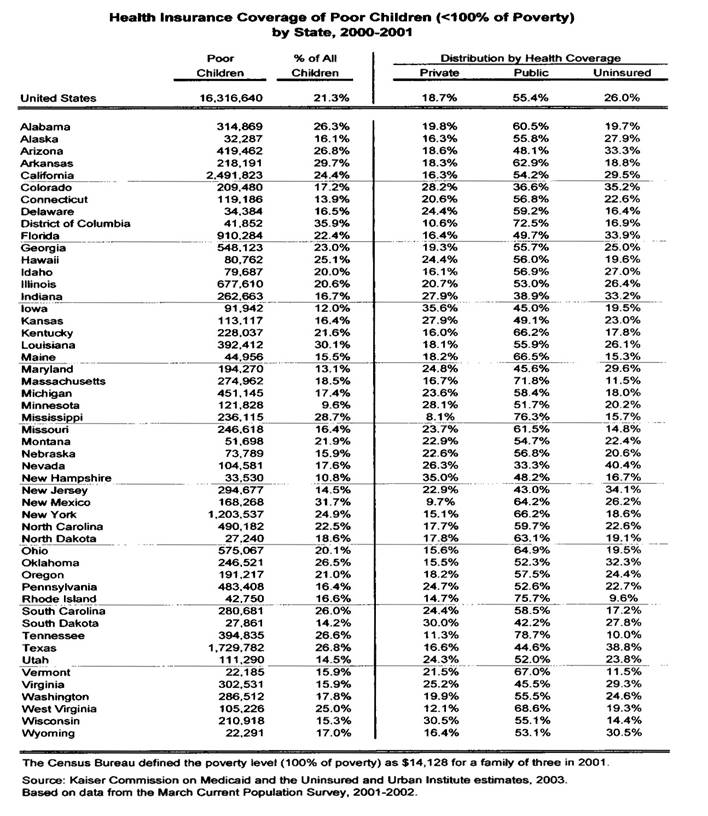
- In 2000-2001, Nevada led the nation in the percentage of poor children (family income <100 FPL) who were uninsured (Figure 3).
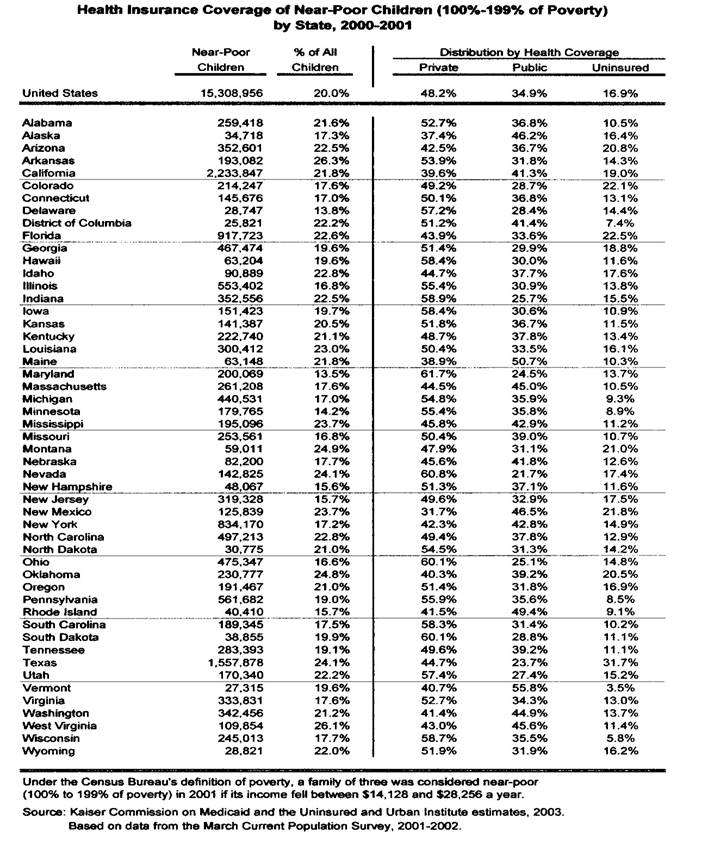
- In 2000-2001, Nevada also led the nation in the percentage of near poor children (family income 100% to 199% FPL) who were uninsured (Figure 4)
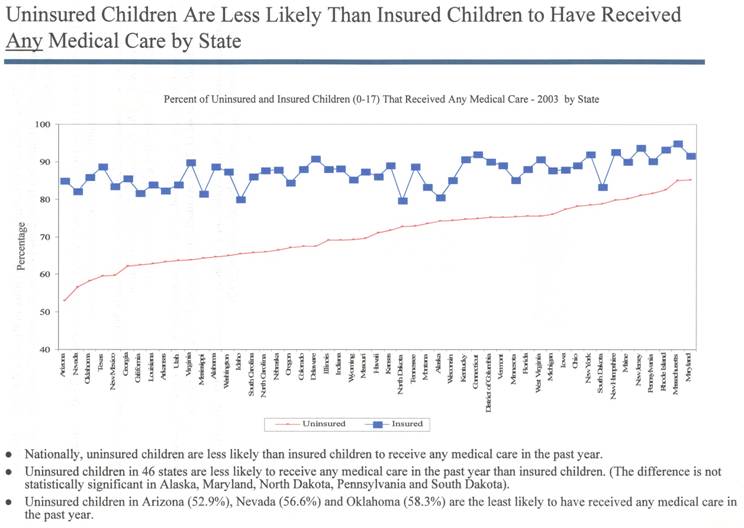
- In 2003, 10.9% of Nevada’s uninsured children did not receive needed medical care. Nevada had the 3rd highest percentage of uninsured children in the nation who did not receive needed care (Figure 5).
- In 2003-2004, over 17% of Nevada’s children were uninsured. The national average was 11.7%.
- The percentage of uninsured children in Nevada has been higher than the national average every year since 1990.
- In 2001, almost 29% of minority/ethnic residents in Nevada were uninsured, ranking Nevada 11th highest in the nation for the percentage of uninsured minority/ethnic residents.
In a report issued by the Nevada Office of Rural Health, http://www.unr.edu/med/dept/CEHSO/orh.html, (University of Nevada School of Medicine, 2004),
- There were no significant differences in the overall average of uninsured persons between urban counties and rural or frontier counties. The percentage of uninsured persons was slightly lower in many of the rural and frontier counties than the urban counties ( Carson City, Clark, and Washoe counties).
- However, Elko, Humboldt and Lander counties had slightly higher numbers of uninsured than the state average.
Several factors contribute to the high number of uninsured in Nevada. Since the early 1990’s, Nevada has been one of the fastest growing states in the United States, and this growth has contributed to the numbers of uninsured in Nevada.
The percent of people covered by Medicaid was consistently lower in Nevada than in the rest of the nation from 1987-2003. (Great Basin Primary Care Association, 2005). Consequently, Nevada has a higher percentage of low income citizens who are uninsured. Despite this, Nevada faces further decline in its Federal Medical Assistance Percentage (FMAP), http://aspe.hhs.gov/health/fmap.htm, in 2006. FMAP is the federal contribution to the Nevada Medicaid program (The Kaiser Commission on Medicaid and the Uninsured, 2005).
- Nevada has seen recent modest gains in its Nevada Check-up (SCHIP) program enrollment. However, federal regulations prevent SCHIP funding to be spent on administrative functions, such as program promotion. Therefore, it has been difficult for the State to get eligible children enrolled in the program.
- Nevada has the 14th largest Hispanic population in the U.S. (National Council of Las Raza, 2005). 40% of this population is under the age of 19 years. 52% percent of Hispanics are native born citizens, 12% are naturalized citizens, and 36% are non-citizens.
Although the Hispanic employment rate is higher than for the total population (74% vs. 67%), Hispanics are more likely to live in poverty. Many Hispanics work for small businesses, family owned businesses, or in occupations that do not provide health insurance. These factors contribute to the high number of Hispanic non-elderly who are uninsured.
- In 2001, 36% of non-elderly Hispanic Nevadans were uninsured, and they represented 40% of the total uninsured in Nevada.
Nevada Public Insurance for Low Income Children
Nevada has two public insurance programs for low income children – Nevada Medicaid, http://dhcfp.state.nv.us/ and Nevada Check Up (Nevada SCHIP program), http://www.nevadacheckup.state.nv.us/. Children who may be eligible for Nevada Medicaid coverage:
- Severely disabled children.
- A child receiving Supplemental Security Income (SSI).
- Children who are born in the United States and who are U.S. citizens.
- Children who are born after September 30, 1983 if they meet an income and assets test.
- Children up to age six years whose family gross income is at or below the 133% federal poverty level (FPL).
- Children age six years and older whose family gross income is at or below 100% of FPL.
Children who may be eligible for Nevada Check Up:
- Child must not be eligible for Medicaid.
- Child must be a U.S. citizen or legal resident.
- Child may not have had health insurance within the last 6 months.
- Child does not have access to the State Public Employee Benefits
- Child must be under age 18 at the date of application for Nevada Check Up.
- Child must be in a family whose household income does not exceed 200% FPL.
Enrollment of low income children in Nevada Medicaid and SCHIP (Kaiser Commission on Medicaid and the Uninsured, 2003; Kaiser Commission on Medicaid and the Uninsured, 2005):
- In 2000-2001, Nevada had the lowest percentage of poor children (<100% FPL) with public insurance coverage (Medicaid and SCHIP) in the nation (Figure 3).
- In 2000-2001, Nevada also had the lowest percentage of near poor children (100%-199% of FPL) with public insurance coverage (Medicaid and SCHIP) in the nation (Figure 4).
- From 2000 to 2004, Nevada ranked 3rd lowest in the nation in the percentage increase in children enrolled in Medicaid (-0.7% decrease in Medicaid enrollment), while it ranked 21st highest in the nation in the increase in uninsured children (0.3% increase in uninsured children).
In 2001, state Medicaid and SCHIP programs with the following features had higher enrollments than other states (Kronebusch and Elbel, 2004):
- Medicaid expansion SCHIP programs rather than Medicaid-SCHIP combination programs or stand alone SCHIP programs (Medicaid expansion programs allow for better SCHIP-Medicaid coordination).
- No assets test, no presumptive eligibility procedure, and no self-declaration of income procedure.
- As of July, 2005, the Nevada SCHIP program was a stand alone program with no joint Medicaid-SCHIP application process, and the Nevada SCHIP and Medicaid programs did not have presumptive eligibility or self-declaration of income procedures.
State Initiatives to Expand Insurance Coverage
States have been taking the lead in expanding coverage to the uninsured. States have undertaken two basic approaches to expanding coverage – reforming their private insurance markets and expanding their public coverage (Fuchs, 2004). Prior to 2000, the states had implemented the following private insurance reforms (the number states that had implemented the reform are given where state data were available):
- Guaranteed plan issue, guaranteed plan availability or open enrollment – 12 states.
- Restrictions on the use of pre-existing conditions, exclusions and waiting periods – 31 states.
- Guaranteed plan renewability (required by COBRA) – 50 states. Rating bands that restrict the difference between the lowest and highest premium that an insurer may charge for the same coverage – 6 states.
- Modified community rating that allows insurers to vary premiums for coverage based on specific demographic characteristics (age, gender, location) – 9 states.
- Pure community rating that allow insurers to vary premiums based only on where the enrollee lives, specific benefit package selected, and the family size – 1 state.
- State is the insurer of last resort.
- State has a high risk pool to provide insurance to individuals who are uninsurable due to having a high cost medical condition.
- State has a reinsurance pool that allows insurer to pass on high risk individuals to a centralized pool of insurers.
In Nevada, the Division of Health Insurance, http://www.nvquote.com/, has implemented a state reinsurance pool, but, to date, no private insurer has joined the pool. Nevada businesses do not believe that the program offers enough protection against risk (Hurst, 2005). In 1991, the Nevada State Senate passed a bill (SB 503),
http://www.leg.state.nv.us/lcb/research/library/1991/SB503,1991.pdf, that allowed insurers to offer basic benefits plans (“bare bones” plans) to small employers to reduce their premiums. There was very little demand for these plans, and SB 503 has since been repealed.
- Nevada has limited ability to reform the employer-based insurance market, because about 65% of Nevadans with employer-based insurance are covered by self funded plans that are not regulated by the Nevada Division of Insurance.
In a recent review of the research on the effectiveness of these state private market reforms, Fuchs (2004) concluded the following:
- Availability of insurance for high risk persons was expanded in the few states that adopted both guaranteed issue and some form of community rating.
- The gains in access to coverage for high risk people were modest, at best, more likely because these reforms did not bring down the cost of insurance low enough to attract large numbers of uninsured.
- More modest state reforms, such as annual open enrollment, rate bands, and high risk pools produced weak or no statistically significant effects on rates of coverage.
The following are the major initiatives that states have undertaken to expand their publicly funded coverage (Austin, et. al, 2205):
- Expanding Medicaid and SCHIP coverage.
- Comprehensive reform programs that target health care costs, quality and access. Maine has the most ambitious of such plans, which has been named Dirigo. Under Dirigo, Maine plans to expand coverage to all Mainers by 2009
- Utilizing Health Insurance Flexibility and Accountability Initiative (HIFA) and Medicaid Section 1115 waivers, http://www.cms.hhs.gov/medicaid/1115/default.asp, to experiment with different approaches to covering their uninsured populations.
- Utilizing Health Resources and Services Administration’s (HRSA) State Planning Grants to study their demographic and health insurance trends to develop coverage options.
- State ballot initiatives to expand coverage in states like California, Colorado, Oklahoma and Montana.
In Nevada, pursuant to State Assembly Bill 493, http://www.leg.state.nv.us/73rd/Bills/AB/ab493.pdf#xml=http://search.leg.state.nv.us/isysquery/irl3e3d/3/hilite, the state Medicaid program is applying for a HIFA waiver that, if granted, would (Nevada State Assembly, 2005):
- Extend Medicaid coverage of pregnant women from the current 133% FPL to 185% FPL.
- Provide a premium subsidy in an amount of $100 per person per month to employees and their spouses: (1) who work for an employer that employs at least 2 but not more than 50 employees, and (2) who has a household income of less than 200% of FPL, and (3) who is otherwise ineligible for Medicaid.
- Provide coverage for hospital care to persons who have low incomes, are otherwise ineligible for Medicaid, and who have a catastrophic illness or injury that results in unpaid charges for hospital care.
Faced with growing Medicaid and SCHIP budgets, most states have endured bad budget years without making deep cuts to Medicaid programs (Austin, et al., 2005). However, state officials worry that their Medicaid programs cannot sustain the current rate of cost increases much longer. A combination of surging costs, enrollment and the uninsured has created a “perfect storm” that has driven many Medicaid leaders to rethink the way their programs are structured and operate.
National Proposals to Expand Insurance Coverage
National proposals to expand insurance coverage, if enacted into law, could impact uninsured Nevadans. During the 2004 presidential campaign, President Bush and Senator Kerry proposed the following policy options to increase insurance coverage (Stumpf and Cubanski, 2005):
- President Bush proposed: (1) tax credits for low income individuals to purchase insurance in the private market, (2) federal tax deduction for individuals who purchase high deductible non group coverage in combination with a Health Savings Account (HSA), (3) tax credit for small businesses and their employees who set up and contribute to an HSA, (4) allowing small businesses and other civic and charitable groups to combine their purchasing power through Association Health Plans (AHPs), and (5) the “Cover the Kids” campaign with the goal of covering all SCHIP-eligible children within the next two years. Bush’s plan is estimated to cost the federal government between $91 billion and $195 billion over 10 years (2005-2014) and provide coverage for approximately two to eight million uninsured persons.
- Senator John Kerry proposed: (1) expanding Medicaid and SCHIP coverage, (2) federal reinsurance against catastrophic costs for health insurance plans provided by the federal government, (3) allowing individuals and employers to buy into the Federal Employees Health Benefits Program (FEHBP). Kerry’s plan is estimated to cost the federal government between $653 billion and $1,305 billion over 10 years (2005-2014) and to cover 25 to 27 million uninsured Americans.
An alternative proposal is a single payer national health insurance program (NHI). Proponents of NHI argue that a more radical reform is needed if we are going to provide affordable, comprehensive insurance coverage to all Americans (Angell, 2005). Under a NHI program, all U.S. citizens would be enrolled into a single, federally funded, comprehensive insurance program, but individuals could still purchase supplemental private policies for non-covered services. All the current government-funded insurance programs would be folded into the NHI program.
Conclusion
Nevada continues to have a relatively high rate of persons without health insurance. Nevada has a higher than national average percentage of uninsured low income adults, low income children and minority residents. Low income, minority adults are uninsured, because they work for businesses that do not provide an insurance benefit; they work for a company that provides a benefit but they cannot afford to purchase the benefit; they are not U.S. citizens; and/or they are not eligible for Nevada’s relatively stringent Medicaid program.
Low income children are uninsured, because many of them are not
enrolled in the Nevada Medicaid and/or the Nevada SCHIP programs.
Compared with other states, Nevada has done very little to expand private insurance coverage to the uninsured, and Nevada is just currently applying for a HIFA waiver to expand Medicaid coverage to the uninsured. In order to reduce its number of uninsured residents, Nevada needs to do more to expand coverage through the private insurance market and to expand coverage through Medicaid and SCHIP.
Data Sources and Suggested Readings
American Association of Retired Persons (2003). State profiles: Reforming the health care system 2003. Retrieved November 25, 2005 from http://www.aarp.org/research/health/carefinancing.
Angell, M. (2005). Proposal of the physician’s working group for single-payer national health insurance. Physicians for a National Health Plan. Retrieved December 2, 2005 from http://www.physiciansproposal.org/embargoed/angell.html.
Austin, B., et al.(2005). State of the states, finding alternate routes. Academy Health. Retrieved December 1, 2005 from http://www.statecoverage.net/pdf/stateofstates2005.pdf.
Benedict, Jennifer (personal communication, January 27, 2006).
DeNavas, W.C., Proctor, B., & Lee, H. (2005). Income, poverty, and health insurance coverage in the United States: 2004. U.S. Census Bureau. Retrieved November 23, 2005 from www.AccreditedOnlineColleges.org.
Fuchs, B.C. (2005). Expanding the individual insurance market: Lessons from the state reforms of the 1990s. The Robert Wood Johnson Foundation. Retrieved December 1, 2005 from http://www.rwf.org/publications/synthesis/reports_and_briefs/pdf/no4_synthesisreport.pd.
Great Basin Primary Care Association (2005). 2005 edition of the Nevada study of uninsured populations. Retrieved ecember 2, 2005 from http://www.gbpca.org/uninsured/.
L. Larry Hurst (personal communication, December 1, 2005).
Institute of Medicine (2004). Insuring America’s health: Principles and recommendations. Retrieved November 22, 2005 from http://www.iom.edu/report.asp?id=17632.
The Kaiser Commission on Medicaid and the Unisured (2003). The health insurance status of low income children and their parents: recent trends in coverage and state level data. Retrieved December 10, 2005 from http://www.kff.org/uninsured/upload/The-Health-Insurance-Status-of-Low-Income-Children-and-Their-Parents-Recent-Trends-in-Coverage-and-State-Level-Data.pdf.
Kronebusch, K. & Elbel, B. (2004). Enrolling children in public insurance: SCHIP, Medicaid and state implementation. Journal of Health Politics, Policy and Law, 29: 451-489.
National Coalition on Health Care (2004). Facts on health insurance coverage. Retrieved November 23, 2005.
National Council of La Raza (2005). Nevada state fact sheet. Retrieved November 25, 2005 from http://www.nclr.org/content/publications/detail/31926/.
Nevada State Assembly (2005). Assembly Bill no. 493. Retrieved December 2, 2005 from http://www.legislative.state.nv.us.
Robert Wood Johnson Foundation (2005). Going without: America’s uninsured children. Retrieved December 10, 2005 from http://coveringkidsandfamilies.org/press/docs/2000SBTResearcjRe[port.pdf.
Stumpf, E.C. & Cubanski, J. (2005). Options for federal coverage of the uninsured in 2005. The Commonwealth Fund. Retrieved December 1, 2005 at http://www.cmwf.org/usr_doc/831_Stumpf_federal.pdf.
The Kaiser Commission on Medicaid and the Uninsured (2005). Health insurance coverage of the non elderly by state, 2003-2004. Retrieved November 23, 2005 from http://www.kff.org/uninsured/kcmu110405pkg.cfm.
University of Nevada School of Medicine, Nevada Office of Rural Health (2004). Nevada rural and frontier health data book, 2004 edition. University of Nevada School of Medicine: Reno, NV.
U.S. Census Bureau (2005). Health insurance data. Retrieved November 21, 2005 from http://www.census.gov/hhes/www/hlthins/hlthinstypes.html.
Community Resources
Nationwide Resources
Commonwealth Fund – the Commonwealth Fund’s mission is to promote a high performing health care system that achieves better access, improved quality and greater efficiency, particularly for society’s more vulnerable, including low income people, the uninsured, minority Americans, young children and elderly adults. The Commonwealth Fund, 1 East 75th Street, New York, N.Y. 10021; Phone: 212-606-3800. Fax: 212-606-3500. Website: http://www.cmwf.org.
Cover the Uninsured Week 2005 – a Robert Wood Johnson Foundation-sponsored national effort to mobilize physicians, employers, policymakers and other stakeholders on behalf of the nation’s 44 million uninsured. Website: http://covertheuninsuredweek.org/. The site includes a downloadable Guide to Finding Health Care Coverage for Nevadans and a downloadable Guide to Health Insurance Options for Small Business.
Kaiser Family Foundation – the Henry J. Kaiser Family Foundation is a non profit, private operating foundation focusing on the major health care issues facing the nation. The Foundation is an independent voice and source of facts and analysis for policymakers, the media, the health care community, and the general public. The Kaiser Family Foundation, 2400 Sand Hill Road, Menlo Park, CA 94 Tel. 650-854-9400. Fax: 650-854-4800. Website: http://www.kff.org.
Physicians for a National Health Plan (PNHP) – PNHP is a national physicians’ organization that is advocating for a single payer, national health insurance program that would provide comprehensive heath care coverage to all Americans. Tel. 312-782-6006; Website: http://www.pnhp.org/.
Nevada Resources
ClarkCounty Social Service Medical Assistance Program – the Medical Assistance Program provides medical care to indigent and medically needy individuals who are not eligible for other public or private programs. The Program also pays COBRA and other private insurance premiums, co-pays and deductibles for some eligible indigent individuals. Eligibility determination is based upon an assessment of need according to established agency guidelines. Clark County Social Service, 1600 Pinto Lane, Las Vegas, NV 89106; Tel. 702-455-4270; fax: 70-455-5950.
Governor’s Office for Consumer Health Assistance – the Office for Consumer Health Assistance was established to provide a single point of contact for consumers and injured workers to assist them in understanding their rights and responsibilities under Nevada law and health care plans, including industrial insurance policies. The Office is dedicated to providing assistance through information, counseling, education and advocacy. Las Vegas, 555 E. Washington Avenue, Suite 4800, Las Vegas, NV 89101; Tel. 702-486-3587; Fax: 702-486-3586; Toll Free Number: 1-888-333-1597; Website: http://www.govcha.state.nv.us/.
Great Basin Primary Care Association – the Great Basin Primary Care Association is a coalition of community-based primary care organizations that have joined together to improve the health status of Nevada’s medically underserved and indigent populations by supporting and advocating on behalf of the community-based health centers, which provide accessible, quality, comprehensive primary care services. Tel. 775-887-0417; Website: http://gbpaca.org/commhealth.htm.
Nevada AIDS Drug Assistance Program (ADAP) – ADAP provides HIV medication to needy individuals with little or no private insurance or Medicaid coverage. Nevada residents who can document their HIV status, have income less then 400% of the FPL, and have other assets worth less than $4,000 (excluding their house or car) are eligible for ADAP assistance. Nevada AIDs Drug Assistance Program, 505 East King Street, Room 103, Carson City, NV 89701; Tel. 775-684-5996; fax: 775-684-4056.
Maternal Child Health Line – the Maternal Child Health (MCH) Line helps pregnant women in Nevada obtain early and continuous prenatal care. The MCH Line can also help with financial assistance, a baby car seat, immunizations and other needs. Tel. 1-800-429-2669.
Nevada Check-up – Nevada Check-Up is the Nevada SCHIP program, and the program provides low-cost, comprehensive health care coverage to low income, uninsured children (birth through 18) who are not covered by private insurance or Medicaid. Phone: 800-360-6044 or 775-684-3777. Para español 800-360-6044 or 775-684-3777. Website: http://www.nevadacheckup.state.nv.us/.
Nevada Division of Insurance – the Division of Insurance provides information and assistance on obtaining health insurance in the State of Nevada, including information on Medicare, Medigap insurance, Health Coverage Tax Credit, and the State Health Insurance Program (SHIP). Carson City Office: 775-687-4270; Las Vegas Office: 702-486-4009. Website: http://www.doi.state.nv.us/.
Nevada Medicaid – The Nevada Medicaid program is located in the Nevada Division of Health Care Financing & Policy (DHCFP). The purpose of the program is to purchase medically necessary health care and related services for Medicaid eligible persons. Nevada Medicaid, 1100 East William Street, Suite 101, Carson City, NV 89701. Tel. 775-684-3676. Fax: 775-687-3893. Website: http://dhcfp.state.nv.us/.
Nevada Senior Rx - Senior Rx provides Nevada seniors with insurance coverage to offset the cost of prescription medication. The program provides up to $5,000 in benefits per year. Many of the most commonly prescribed drugs are available for a co-pay of $10 per drug. Website: http://dhhs.nv.gov/seniorrx.htm. Tel. 1-866-303-6323.
Nevada’s Vaccines for Children (VFC) – Vaccines for Children is a federally funded vaccine supply program. VFC-provided vaccines can be given to all children, 18 years of age or younger. Nevada’s VFC program, however, was initiated to specifically cover children who are Medicaid eligible, do not have health insurance, are not covered for immunizations by their health insurance plan, and/or American Indian or native Alaskan. Tel. 775-684-5900 Website: http://health2K.state,nv.us/vfc/.
Nevada Women’s Health Connection – The Women’s Health Connection is a breast and cervical cancer early detection program available to women age 40 and above who do not have Medicaid or Medicare Part B, are not a member of an HMO, or are uninsured or underinsured and meet the income eligibility guidelines. Department of Human Resources, Health Division, 505 East King Street, Room 103, Carson City, NV 89701; phone: 1-888-463-8942; Website:
http://health2K.state.nv.us/whc/.
This report was prepared by Dr. Charles Moseley, Associate Professor and Chair, Department of Health Care Administration and Policy (HCAP), School of Public Health, University of Nevada, Las Vegas (UNLV) and Michelle Sotero, Graduate Assistant, Department of HCAP. Dr. Moseley can be contacted at: Surface mail: Department of HCAP, UNLV, 4505 Maryland Parkway, Box 453023, Las Vegas, NV 89124-3023. Phone: 702-895-4413. Fax: 702-895-5184. Email: charles.moseley@unlv.edu.